1. What "fasting" actually means.
Fasting is not one thing. The word covers everything from shortening your daily eating window by two hours to not eating for seven days. Lumping them together is the single most common mistake in popular fasting writing — the protocols do different things to your body, take different effort, and carry very different risks. Before anything else, get the terminology straight:
| Term | What it actually means |
|---|---|
| Time-restricted eating (TRE) | All your calories in a defined daily window (typically 6–12 hours). Common shapes: 16:8 (16h fast + 8h window), 14:10, 12:12. Most-studied form of intermittent fasting in modern human trials. |
| Intermittent fasting (IF) — umbrella | Used loosely. In the academic literature it covers TRE, alternate-day fasting, and 5:2 — i.e., any pattern of regular eating + regular not-eating. |
| Alternate-day fasting (ADF) | One day eat freely, next day eat ~500 kcal (or nothing). Repeat. Better data than its reputation; harder to sustain than TRE. |
| 5:2 | Five normal eating days per week, two non-consecutive days at ~500 kcal each. Popularized by Mosley; clinically similar to ADF in effect. |
| Prolonged fasting | Water-only (sometimes black tea/coffee) for ≥3 days, often 5–7 days. Real risks; should not be done casually. |
| Fasting-mimicking diet (FMD) | A 5-day, ~800–1,100 kcal/day plant-based diet engineered to reproduce the molecular signatures of water fasting (low IGF-1, high ketones) while delivering enough nutrients to be safe ambulatory. Branded as ProLon by Valter Longo's group; the clinical trials are FMD-specific[12,14]. |
The single best plain-English review of this whole field is de Cabo & Mattson's 2019 paper in the New England Journal of Medicine — open access, written for clinicians but readable[1]. If you only read one outside source after this page, read that one.
2. The 24-hour metabolic timeline.
Your body doesn't "start fasting" at any one clock time. It moves through a sequence of fuel-source shifts as the hours since your last meal stack up. Understanding the rough order matters because most of the benefits people associate with fasting — fat burning, ketones, autophagy — sit at different points along this timeline[1,2].

0–4 hours after eating: digesting and absorbing. Insulin is up, glucose is being pushed into muscle and liver. You're storing fuel, not using it. Almost no fat burning.
4–12 hours: post-absorptive / early fasted. Insulin starts to drop. Liver glycogen is broken down (glycogenolysis) to maintain blood glucose. Fat starts being released from fat cells (lipolysis) and used.
12–18 hours: the metabolic switch. Liver glycogen runs low. The body shifts substantially to fat as primary fuel. Ketones — small water-soluble fuel molecules made by the liver from fat — start measurably rising. This is the boundary Anton et al 2018 named "flipping the metabolic switch"[2].
18–24 hours: ketosis deepening. Ketones (mainly β-hydroxybutyrate) become a significant fuel for brain, heart, and muscle. Growth hormone rises modestly. Insulin is at its low. Autophagy markers begin to climb in animal models; the human evidence is less clean (more in §4).
24–72 hours: prolonged fasting territory. Ketones peak around 48–72 hours. IGF-1 drops substantially. Stem-cell signaling shifts — the Cheng 2014 work in Cell Stem Cell showed prolonged fasting cycles drove hematopoietic-stem-cell-based regeneration and partially reversed chemotherapy-induced immunosuppression in mice + correlative human findings[13].
Beyond 72 hours: real prolonged fast. Continued ketone elevation, deeper IGF-1 suppression, gradual decrease in basal metabolic rate, electrolyte management becomes mandatory. This is the territory where serious risks (refeeding syndrome, electrolyte imbalance, dehydration) appear, and where the literature transitions from "self-experimentation" to "clinical supervision required."
3. The glucose-to-ketone switch.
Your brain is the world's most metabolically expensive organ — about 20% of your resting energy use, even though it's only 2% of your weight. By default it runs on glucose. But when glucose runs low, the liver makes ketones — small water-soluble fuel molecules that cross the blood-brain barrier and substitute for glucose in the brain. This switch is what makes prolonged fasting compatible with consciousness and survival.

Three ketone bodies are produced:
- β-hydroxybutyrate (BHB) — the most abundant in blood, the one consumer blood-ketone meters measure. Levels of 0.5–3 mmol/L are typical nutritional ketosis; >3 mmol/L starts to look like prolonged-fast territory; 5+ mmol/L appears around day 3–4 of a water fast.
- Acetoacetate (AcAc) — the immediate ketogenic product; spontaneously decarboxylates into acetone.
- Acetone — exhaled through the lungs. The source of the "fruity" or "nail-polish" breath people notice in deep ketosis.
Three hormonal moves drive the switch. Insulin falls: with no food coming in, the pancreas stops releasing insulin, removing the brake on fat release from adipose tissue. Glucagon and catecholamines rise: signaling the liver and fat cells to mobilize stored energy. Growth hormone rises modestly: helping preserve muscle mass during the fast. The net effect is a body that is biochemically very different from its fed state — and most of fasting's downstream effects (metabolic health, autophagy, weight loss) trace back to this hormonal pattern[1,2].
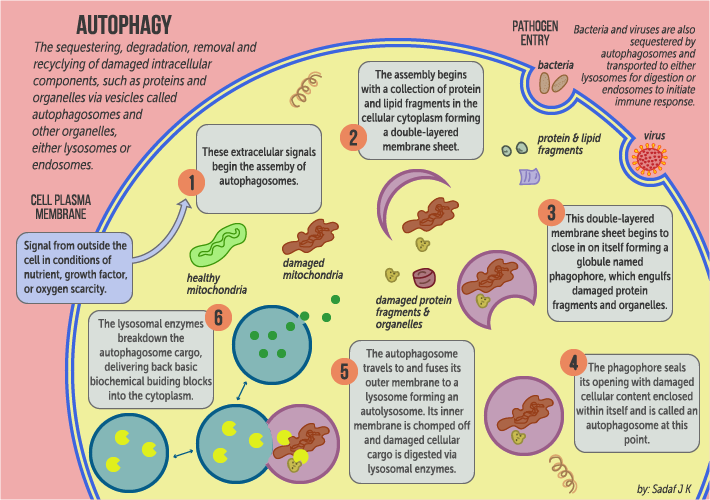
4. Autophagy — what it actually is, and when it starts.
Autophagy — literally "self-eating" in Greek — is the cellular process that breaks down damaged proteins, worn-out organelles, and accumulated junk inside cells, then recycles the components back into building blocks. It is to a cell what cleaning out the garage is to a household: a maintenance process that runs continuously at low levels and ramps up when resources are scarce. The 2016 Nobel Prize in Physiology or Medicine went to Yoshinori Ohsumi for working out the genetic machinery. The standard plain-English review is Mizushima & colleagues' 2008 Nature paper[3].
The internet's "autophagy starts at 16 hours" claim is overstated. Autophagy runs continuously at a low baseline rate in every cell of your body. What changes with fasting is the rate, and what changes that rate is two signaling pathways:
- mTOR — the cell's "build and grow" master switch. Active when amino acids and insulin are high (fed state); suppressed when food is absent. mTOR suppression is the direct trigger to ramp autophagy up.
- AMPK — the cell's "energy low" sensor. Active when ATP is low / AMP is high (fasted, depleted, exercised state). AMPK activation also ramps autophagy up.
Both pathways shift gradually during a fast — they don't flip on at a clock time. The strongest direct measurements of autophagy come from animal studies (where you can biopsy tissue) and not from humans (where you mostly can't). The honest summary: autophagy markers increase progressively across a fast, with the bigger shifts at the 24-hour-and-beyond mark rather than at the 16-hour mark — but exact dose-response in humans is still being worked out[1,3].
What this means practically: if autophagy is your goal, the strongest evidence sits at the prolonged-fast or FMD end of the spectrum, not at 16:8. 16:8 still has metabolic and weight benefits — but selling 16:8 specifically as an "autophagy intervention" is overpromising compared to the actual evidence base.
5. Insulin sensitivity and glucose regulation.
This is where the modern human-trial evidence is cleanest. Insulin sensitivity — how effectively your cells respond to insulin to clear glucose from blood — is the single most important upstream lever for type 2 diabetes, metabolic syndrome, and most cardiovascular risk. Several well-designed RCTs have asked whether time-restricted eating moves it.
The cleanest answer comes from Sutton et al's 2018 Cell Metabolism trial. Eight men with prediabetes were randomized to either early time-restricted feeding (eTRF) — 6-hour eating window ending before 3pm — or a 12-hour control window, both for 5 weeks, then crossed over. Caloric intake was matched between arms. Insulin sensitivity improved, blood pressure dropped, and oxidative-stress markers fell on the eTRF arm even though no weight was lost. The window shape mattered — not just the calorie intake[4].
Wilkinson et al's 2020 Cell Metabolism trial extended this to metabolic-syndrome patients on a more practical 10-hour eating window for 12 weeks. Result: weight, blood pressure, and atherogenic lipids all dropped — without specific caloric prescription[9]. Gabel et al 2019 found alternate-day fasting was more effective than daily calorie restriction at lowering insulin resistance specifically, despite similar weight loss[11].
The synthesis: fasting protocols improve insulin sensitivity at least partly through mechanisms independent of weight loss. If improving your metabolic markers is the goal, the early-window shape (eating done by 3–6pm) has the best data — and it works even without losing weight.
6. Weight loss — what the RCTs actually show vs the marketing.
For weight loss specifically, the trial evidence is more deflationary than the marketing. The three largest, best-designed trials all point to the same conclusion: fasting protocols work for weight loss to the extent that they create a sustained calorie deficit — they are not magic above and beyond their calorie effect.
The TREAT trial (Lowe et al 2020, JAMA Internal Medicine) randomized 116 adults with overweight or obesity to either standard 3-meals-a-day OR time-restricted eating (16:8 with a noon–8pm window). After 12 weeks, weight loss on the 16:8 arm was modest (~0.94 kg) and not significantly different from the control arm. The 16:8 group also lost more lean mass than expected[5]. Lowe's trial deserves both the credit for being rigorous and the caveat that it used a late eating window (the metabolically-weaker shape, per §5).
The Trepanowski 2017 JAMA Internal Medicine trial randomized 100 obese adults to alternate-day fasting, daily calorie restriction, or no intervention for one year. At one year: ADF and CR produced essentially identical weight loss (~6%); the ADF arm had higher dropout, suggesting it was harder to sustain[6]. The Liu 2022 NEJM trial took it further — randomized 139 obese adults to calorie restriction alone vs calorie restriction + time-restricted eating for 12 months. Weight loss at 12 months was the same in both groups (~8 kg). The extra TRE constraint added nothing once calories were controlled[7].
The Jamshed 2022 JAMA Internal Medicine trial is the most recent and the most-cited counter-data: 90 obese adults, 14 weeks, randomized to early TRE (8-hour eating window before 4pm) + standard calorie deficit OR standard calorie deficit alone. The early-TRE arm lost about 2 kg more — modest but statistically significant[10]. Consistent with §5: window shape matters; early is better than late.
The honest synthesis: If weight loss is your only goal, fasting protocols are about as effective as straightforward calorie restriction. Some people find a defined eating window easier to comply with than counting calories — and that's the legitimate reason to pick one. Picking 16:8 expecting that it will somehow override the energy-balance arithmetic is not what the trials support[5,6,7,8,10].
7. Protocols, with their actual rules.
12:12 — start here if you've never fasted.
Rules: no calories between, say, 8pm and 8am. Best for: complete beginners. Cautions: minimal; almost everyone tolerates 12:12 within days. RCT data: limited as a standalone (most trials use 14h or longer windows) but Anton 2018 frames 12:12 as the natural starting point for the metabolic switch[2].
14:10 — the realistic adoption-friendly target.
Rules: 14h fast, 10h eating window. Best for: anyone with a rigid social/family schedule who can't realistically hit 16:8. Cautions: mild adaptation period. RCT data: Wilkinson 2020 used 10h TRE in metabolic-syndrome patients — meaningful drops in weight, BP, and atherogenic lipids over 12 weeks[9].
16:8 — the modern default TRE protocol.
Rules: 16h fast, 8h eating window. Common shapes: 12pm–8pm (late TRE) or 8am–4pm (early TRE). Best for: anyone wanting the most-studied IF protocol. Cautions: late-TRE works for weight loss but the metabolic-marker data is much better for early-TRE — see Sutton 2018 (eTRF in prediabetes) and Jamshed 2022 (early-TRE beats late for fat loss)[4,10].
5:2 — five normal days, two ~500-kcal days.
Rules: five days unrestricted, two non-consecutive days at ~500 kcal (women) or ~600 kcal (men). Best for: people who hate the daily window but can do two structured low-cal days. Cautions: easy to overeat on non-fast days. RCT data: Trepanowski 2017 found ADF and CR equivalent for weight at 1 year; 5:2 by extension performs similarly when adherence is matched[6].
Alternate-day fasting (ADF) — one day on, one day off.
Rules: alternate eating-day and fasting-day (or modified fast with ~500 kcal). Best for: people willing to make a single big restriction every other day. Cautions: higher dropout in trials than TRE — sustainability is the bottleneck. RCT data: Trepanowski 2017 (1-year RCT, ADF vs CR vs control)[6]; Gabel 2019 (ADF improved insulin resistance more than CR at equal weight loss)[11].
Prolonged fast (3–5 days water-only) — real benefits, real risks.
Rules: water (and usually black coffee/tea, salt) only for 3–5+ days. Best for: people exploring the autophagy / IGF-1 / stem-cell signaling lane. Cautions: do not attempt without research — electrolyte management (sodium, potassium, magnesium) is mandatory; refeeding syndrome is real; medication interactions (insulin, blood pressure meds) require physician supervision. RCT data: Cheng 2014 in Cell Stem Cell documented stem-cell-based immune system regeneration; chemotherapy-protection results in animal models replicated in small human cohorts[13].
Fasting-mimicking diet (FMD / ProLon) — the safest prolonged-fast surrogate.
Rules: 5 days of a specific ~800–1,100 kcal/day plant-based diet engineered to reproduce the molecular signatures of water fasting. Best for: people who want the prolonged-fast biological signal (low IGF-1, high ketones, autophagy ramp) without the safety overhead of water-only. Cautions: only the commercial ProLon product has been used in the pivotal trials — homemade approximations may not reproduce the same biomarker shifts. RCT data: Wei 2017 Sci Transl Med — three FMD cycles over 3 months reduced body weight, body fat, blood pressure, and IGF-1 in healthy participants, with a 5-month follow-up showing the changes persisted[12].
8. The fasting-mimicking diet — what it does that water fasting doesn't.
Valter Longo's group at USC engineered the fasting-mimicking diet (FMD) to deliver the molecular benefits of prolonged fasting in a safer ambulatory format. The 5-day FMD provides ~800–1,100 kcal/day from a specific plant-based macronutrient mix (high fat, low protein, modest carbohydrate). The composition is calibrated to keep insulin and amino-acid signaling sufficiently low that the body still enters a fasting-like physiology — low IGF-1, elevated ketones, stem-cell signaling — while delivering enough nutrients to be safe outside a clinical setting.
The pivotal human trial: Wei et al 2017 Sci Transl Med. 100 healthy adults randomized to 3 monthly cycles of 5-day FMD or to continue their normal diet. At the end of 3 cycles: significant reductions in body weight, body fat, blood pressure, fasting glucose, triglycerides, total cholesterol, IGF-1, and C-reactive protein. At a 5-month follow-up after stopping FMD, most of the benefits persisted (compared to baseline). Subjects with the worst baseline markers showed the biggest improvements[12].
Practical considerations. The commercial ProLon product (the FMD as packaged and sold) is what the trials used; homemade approximations exist but the published biomarker data is for the specific formulation. Twice-yearly is a conservative cadence with documented safety. People on diabetes medications, blood-pressure medications, or other prescriptions need physician oversight when fasting at this depth.
9. Fasting and autoimmune disease — the real evidence.
The autoimmune-fasting literature is one of the most exciting and one of the most over-extrapolated areas of the field. The honest read: there is genuinely interesting mechanistic and early human evidence that periodic fasting (specifically FMD) can dampen autoimmune activity, mostly built from one impressive 2016 paper. The translational story has not yet matured into the kind of large RCT evidence that would let any clinician say "fast for your MS." But it is real evidence, and it deserves a careful reading.
The mechanism: clearing damaged immune cells.
Prolonged fasting (3+ days) and the FMD both trigger a controlled depletion of older, more dysfunctional immune cells (especially in the lymphocyte pool), followed by hematopoietic-stem-cell-driven regeneration of fresh ones when food returns. Cheng et al's 2014 work in Cell Stem Cell demonstrated this in mice: cycles of prolonged fasting reduced circulating lymphocytes during the fast, then increased hematopoietic-stem-cell activity, and the regenerated immune system was functionally improved — protecting against chemotherapy-induced damage[13]. If you swap out "chemo damage" for "autoimmune mis-priming," the same regenerative cycle is hypothetically attractive for autoimmune disease.
The mouse + human autoimmune trial: Choi 2016 EAE.
Choi et al's 2016 Cell Reports paper is the keystone autoimmune-fasting study[14]. The paper had two parts:
- Mouse model (EAE, the standard MS analogue): Three cycles of a 3-day FMD significantly reduced disease severity and progression. In some treated mice, FMD completely reversed EAE. Mechanistically: depletion of autoimmune T cells during the fast, then regeneration of oligodendrocyte precursor cells and partial remyelination on re-feeding.
- Pilot human cohort (n=60 relapsing-remitting MS patients): A 7-day modified fast at the start of a 6-month Mediterranean-diet intervention showed signals of improved quality of life and physical-component scores vs control. Underpowered for clinical endpoints, but consistent with the mouse direction.
What this means, and what it doesn't.
The Choi 2016 paper is genuine, replicable in the mouse arm, suggestive in the human arm. It has spawned ongoing trials in MS, rheumatoid arthritis, lupus, IBD, and psoriasis. But:
- The human cohort was small. The clinical endpoints were soft. Larger phase 2 / phase 3 trials are not yet complete.
- "Fasting can dampen autoimmune disease" is not the same as "fasting cures MS" — and the latter is what gets posted online.
- For an active, severe autoimmune flare, stopping standard immunomodulators to "try fasting" is dangerous. The honest sequencing is: keep the standard medical care, add FMD cycles as an adjunct only after discussing with your rheumatologist / neurologist / dermatologist.
- The cross-cluster connection from the gut-microbiome and vitiligo guides is real — autoimmune diseases share immune-system architecture, and interventions that reset that architecture (FMD, fecal microbiota work, JAK inhibitors) tend to be active across multiple autoimmune conditions. But the cross-extrapolation from MS to thyroid disease to vitiligo to RA is mechanistic optimism, not yet trial-confirmed.
The bottom line: FMD has the most defensible autoimmune-fasting case of any protocol; water-only prolonged fasting is more drastic with less specific autoimmune data; and 16:8 TRE has interesting metabolic data but nothing approaching autoimmune-specific evidence. If autoimmune disease is your goal, FMD cycles (under physician oversight) is the lane to discuss with your specialist — not daily TRE.
10. Who should not fast — contraindications.
For some people, structured fasting is dangerous, harmful, or contraindicated. The list is short and worth memorizing.
- Pregnancy and breastfeeding. Caloric and nutrient needs are elevated; restricting intake is harmful to fetal/infant development. Do not attempt structured fasting during pregnancy or while nursing.
- Type 1 diabetes. Fasting without exogenous insulin adjustment can cause both hypoglycemia and dangerous hyperglycemia / ketoacidosis. Any fasting protocol in T1D must be managed by an endocrinologist who can prescribe and adjust insulin doses accordingly.
- History of an eating disorder (anorexia, bulimia, BED). Structured restriction can re-trigger disordered patterns even when framed as "intermittent fasting" — the cognitive overlap is too close. Work with your treating clinician before any intentional restriction.
- Underweight (BMI < 18.5). Loss of further mass is the wrong direction. Address the underlying cause of low weight first.
- On insulin, sulfonylureas, or SGLT2 inhibitors. Real hypoglycemia and euglycemic DKA risks. Medication doses need adjustment by your prescriber before any structured fast; do not "just skip meals" on these.
- Children and adolescents with normal growth trajectories. Restriction can interfere with growth and development.
Beyond the absolute contraindications, several conditions call for slow, supervised introduction: type 2 diabetes on glucose-lowering medications, frailty or sarcopenia in older adults, history of low blood pressure, high-volume training athletes. None of these is an absolute "do not fast" — but each is a "talk to your clinician first" condition[1].
11. How to actually start — practical mechanics.
Ramp don't jump. The most common reason people abandon fasting in week 1 is overshooting on day 1. Start at 12:12 for a week, move to 14:10 the next week, then 16:8 only if the easier windows feel comfortable. Most people adapt within 3 weeks; pushing into discomfort gains nothing biologically and costs the habit.
What breaks a fast, what doesn't. Water: doesn't break a fast. Black coffee or unsweetened tea: doesn't break a fast in any meaningful metabolic sense — they're stimulants, not calories. Salt and electrolytes (no added sugar): essential for fasts >24h, do not break the fast in any relevant biological sense. Sugar-free sweeteners: a grey area — most do not trigger insulin meaningfully but some people get a cephalic-phase insulin response; if your goal is metabolic, default to plain water. Bone broth or anything with calories: breaks the fast — it's still useful for prolonged-fast safety but counts as a partial refeed.
Breaking fasts safely. After 24h+: start with a small protein + low-carb meal (eggs, soup, fish), wait 60 minutes, then a normal meal. After 3–5 day fasts: the first day post-fast should be small portions of easily digested food (vegetable soup, eggs, yogurt) — not a buffet. Refeeding syndrome (electrolyte shifts, especially phosphate and potassium) is a real risk after prolonged fasts.
Electrolytes for fasts ≥24h. Sodium 2–3 g/day (≈1 tsp salt), magnesium 200–400 mg, potassium from supplements or LMNT-style packets. The "keto flu" of mid-fast headache, fatigue, lightheadedness is overwhelmingly electrolyte-driven, not "toxins."
Exercise during fasted state. Light to moderate aerobic work is fine and may even enhance fat oxidation. Strength training in a fasted state is OK if you're experienced but may be suboptimal — for serious lifters, schedule heavy sessions in the fed window or eat 30–60 min after finishing. On prolonged-fast days (3+ days), reduce to walking and mobility work.
Sleep is non-negotiable. Poor sleep undoes most of fasting's metabolic benefits and amplifies the irritability. If you can't sleep 7+ hours during a fasting protocol, fix sleep first and add fasting later.
12. Common myths — what the evidence actually says.
"Fasting destroys your muscle."
Mostly false. Protein-sparing mechanisms (elevated growth hormone, ketone-driven nitrogen sparing) protect muscle during short fasts. The Lowe 2020 TREAT trial did show greater lean-mass loss on 16:8 vs control, but the absolute amount was small (~1.6 kg over 12 weeks) and likely reflected inadequate protein intake during the eating window, not fasting per se[5]. The practical fix is straightforward: hit your protein target (1.6–2.2 g/kg/day) during the eating window and keep resistance training in.
"Fasting damages your metabolism."
False for short fasts; partially true for prolonged extreme restriction. Time-restricted eating up to 16:8 does not measurably reduce resting metabolic rate. Prolonged severe caloric restriction (months-long very-low-calorie diets) does lower RMR — but that's an effect of chronic large deficits, not of an 18-hour overnight fast.
"You need 16+ hours for autophagy."
Overstated. Autophagy runs continuously and increases gradually during a fast; there is no clean dose threshold from human data. The strongest measured autophagy effects come from prolonged fasts and FMD, not 16:8 (see §4).
"Coffee breaks a fast."
False for plain black coffee. Caffeine triggers a small adrenaline response but doesn't meaningfully raise insulin or interrupt the fasted state. Cream, sugar, MCT oil, and bulletproof additions do break the fast.
"Women shouldn't fast."
Oversimplified. There's a kernel of truth — women in the lean-athlete category, women trying to conceive, and women with menstrual-cycle irregularities should be cautious with aggressive fasting because caloric and energy-availability deficits can disrupt the HPA axis and menstrual cycle. But for the average woman with overweight or metabolic-marker goals, the trial evidence (Wilkinson 2020, Lowe 2020, Cienfuegos 2020) includes women and shows benefits comparable to men. The right framing: pay attention to your own cycle and signs, not to a blanket prohibition[5,8,9].
13. Where to start? An interactive protocol matcher.
Fifteen items mapped to the goals, schedule, contraindications, and experience above. Tick what's true for you. Instead of a single 0–15 score, the matcher returns a recommended starter protocol with cautions specific to your answers, and a hard-stop block if any contraindication is checked. Nothing is sent anywhere; the answers are saved only to your own browser so you can revisit and update.
Tick what's true for you. Instead of a single score, the panel below produces a recommended starter protocol matched to your goals, schedule, and experience — with cautions specific to your answers and a hard-stop if any contraindication is checked. Saved to this browser only; nothing is submitted anywhere.
16:8 with a noon–8pm or 11am–7pm eating window
Check at least one item below to see a recommendation.
- Quality of the eating-window calories matters as much as the window length. Use the 16h to fast — not to skip-meal-then-overcompensate.
- Weight (weekly, same time of day)
- Waist circumference (monthly)
- Energy, sleep, and mood (subjective, but write it down — these matter more than the scale early on)
References.
Every PMID below has been verified against PubMed before this page was committed. Click any number in square brackets above to jump to its entry below; click "PubMed" to open the paper.
- de Cabo R, Mattson MP. Effects of Intermittent Fasting on Health, Aging, and Disease. N Engl J Med. 2019;381(26):2541–2551. PubMed: 31881139
- Anton SD, Moehl K, Donahoo WT, Marosi K, Lee SA, Mainous AG, Leeuwenburgh C, Mattson MP. Flipping the Metabolic Switch: Understanding and Applying the Health Benefits of Fasting. Obesity (Silver Spring). 2018;26(2):254–268. PubMed: 29086496
- Mizushima N, Levine B, Cuervo AM, Klionsky DJ. Autophagy fights disease through cellular self-digestion. Nature. 2008;451(7182):1069–1075. PubMed: 18305538
- Sutton EF, Beyl R, Early KS, Cefalu WT, Ravussin E, Peterson CM. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. Cell Metab. 2018;27(6):1212–1221.e3. PubMed: 29754952
- Lowe DA, Wu N, Rohdin-Bibby L, Moore AH, Kelly N, Liu YE, Philip E, Vittinghoff E, Heymsfield SB, Olgin JE, Shepherd JA, Weiss EJ. Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men With Overweight and Obesity: The TREAT Randomized Clinical Trial. JAMA Intern Med. 2020;180(11):1491–1499. PubMed: 32986097
- Trepanowski JF, Kroeger CM, Barnosky A, Klempel MC, Bhutani S, Hoddy KK, Gabel K, Freels S, Rigdon J, Rood J, Ravussin E, Varady KA. Effect of Alternate-Day Fasting on Weight Loss, Weight Maintenance, and Cardioprotection Among Metabolically Healthy Obese Adults: A Randomized Clinical Trial. JAMA Intern Med. 2017;177(7):930–938. PubMed: 28459931
- Liu D, Huang Y, Huang C, Yang S, Wei X, Zhang P, Guo D, Lin J, Xu B, Li C, He H, He J, Liu S, Shi L, Xue Y, Zhang H. Calorie Restriction with or without Time-Restricted Eating in Weight Loss. N Engl J Med. 2022;386(16):1495–1504. PubMed: 35443107
- Cienfuegos S, Gabel K, Kalam F, Ezpeleta M, Wiseman E, Pavlou V, Lin S, Oliveira ML, Varady KA. Effects of 4- and 6-h Time-Restricted Feeding on Weight and Cardiometabolic Health: A Randomized Controlled Trial in Adults with Obesity. Cell Metab. 2020;32(3):366–378.e3. PubMed: 32673591
- Wilkinson MJ, Manoogian ENC, Zadourian A, Lo H, Fakhouri S, Shoghi A, Wang X, Fleischer JG, Navlakha S, Panda S, Taub PR. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell Metab. 2020;31(1):92–104.e5. PubMed: 31813824
- Jamshed H, Steger FL, Bryan DR, Richman JS, Warriner AH, Hanick CJ, Martin CK, Salvy SJ, Peterson CM. Effectiveness of Early Time-Restricted Eating for Weight Loss, Fat Loss, and Cardiometabolic Health in Adults With Obesity: A Randomized Clinical Trial. JAMA Intern Med. 2022;182(9):953–962. PubMed: 35939311
- Gabel K, Kroeger CM, Trepanowski JF, Hoddy KK, Cienfuegos S, Kalam F, Varady KA. Differential Effects of Alternate-Day Fasting Versus Daily Calorie Restriction on Insulin Resistance. Obesity (Silver Spring). 2019;27(9):1443–1450. PubMed: 31328895
- Wei M, Brandhorst S, Shelehchi M, Mirzaei H, Cheng CW, Budniak J, Groshen S, Mack WJ, Guen E, Di Biase S, Cohen P, Morgan TE, Dorff T, Hong K, Michalsen A, Laviano A, Longo VD. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and cardiovascular disease. Sci Transl Med. 2017;9(377):eaai8700. PubMed: 28202779
- Cheng CW, Adams GB, Perin L, Wei M, Zhou X, Lam BS, Da Sacco S, Mirisola M, Quinn DI, Dorff TB, Kopchick JJ, Longo VD. Prolonged fasting reduces IGF-1/PKA to promote hematopoietic-stem-cell-based regeneration and reverse immunosuppression. Cell Stem Cell. 2014;14(6):810–823. PubMed: 24905167
- Choi IY, Piccio L, Childress P, Bollman B, Ghosh A, Brandhorst S, Suarez J, Michalsen A, Cross AH, Morgan TE, Wei M, Paul F, Bock M, Longo VD. A Diet Mimicking Fasting Promotes Regeneration and Reduces Autoimmunity and Multiple Sclerosis Symptoms. Cell Rep. 2016;15(10):2136–2146. PubMed: 27239035
Related on Aayushnitya
- Fasting Window Calculator →
Punch in your eating window and see your fasted hours, ketone-zone hours, and the calendar shape of your week. Companion calculator for the §7 protocols.
- GKI (Glucose-Ketone Index) Calculator →
If you're tracking blood glucose and BHB on a meter, GKI is the single number that summarizes how deep into the fasting/keto state you are. Read it on the GKI chart (ranges, levels, and the autophagy timeline). Useful for prolonged-fast and FMD tracking.
- Caffeine Half-Life Calculator →
Black coffee doesn't break a fast (§ above), but late caffeine wrecks the sleep that makes fasting sustainable. Plot your caffeine decay curve and find your cutoff time.
- CGM Beginner Playbook →
Wearing a CGM during your first fasting protocol gives you a much clearer view of your insulin response than blood tests every few months. The early-TRE evidence becomes visible in your own data.
- Gut Microbiome Guide →
Time-restricted eating shifts microbiome composition meaningfully (the microbiome has a circadian rhythm too). The autoimmune cluster covered in §9 here overlaps directly with the gut-immunity material there.
- Vitiligo Guide →
The autoimmune crossover. Vitiligo's mechanism (CD8⁺ T cells, IFN-γ) overlaps with the immune-cell-clearing rationale for FMD in §9 here; targeted JAK inhibitors and FMD cycles both target overactive autoimmune signaling, from different angles.
This guide is a synthesis of peer-reviewed research and is not medical advice. Fasting interacts with medications and underlying conditions in ways that need clinical oversight — particularly for diabetes, blood-pressure medications, pregnancy, eating-disorder history, and any autoimmune disease covered in §9. The interactive matcher is a starting framework for a conversation with your clinician, not a prescription.