1. The honest headline, first.
Vitiligo is an autoimmune disease in which the body's own killer T cells destroy melanocytes — the pigment cells in the skin. (The mechanism, subtypes, and treatments are covered in depth in the companion Vitiligo guide.) That one fact sets the ceiling on what diet can do: no eating pattern switches the immune attack off, and no food rebuilds destroyed pigment cells. The drugs and phototherapy that actually move the needle work by quieting the immune signalling (JAK inhibitors) or stimulating the surviving melanocyte reservoir (NB-UVB).
Every serious review of nutrition in vitiligo lands on the same sentence: dietary intervention "cannot be thought of as a standalone therapy" and is at best adjunctive[3,4,5,6]. The 2024 systematic review screened 214 studies and found only 14 that met inclusion criteria — and even those mostly describe associations, not interventions that repigment skin[4].
So why a diet guide at all? Because three things are genuinely worth doing, and the internet drowns them under a dozen things that aren't:
- Correct real, measured deficiencies — vitamin D and B12/folate are over-represented in vitiligo (§3).
- Lower the oxidative load — the one mechanistically defensible dietary lever (§2, §4).
- Use the supplement adjuncts that have actual trial data — and only as add-ons to phototherapy (§6).
2. Why diet might matter — the oxidative-stress lever.
There is exactly one mechanism that makes the food–vitiligo link biologically plausible, and it's worth understanding precisely so you can tell the signal from the noise. Vitiligo melanocytes — and the skin around them — carry an abnormally high oxidative burden: elevated hydrogen peroxide (H₂O₂) and reactive nitrogen species that damage the cellular machinery making melanin[2]. The current synthesis is a two-step story: oxidative stress damages the melanocyte first, which flags it as "abnormal" to the immune system, and the immune system then finishes the job.
That's the opening for diet. A pattern rich in dietary antioxidants — polyphenols, carotenoids, vitamins C and E — and low in pro-oxidant inputs (ultra-processed food, excess alcohol, smoking) plausibly lowers the systemic oxidative tone that the melanocyte is fighting against[3,5,6]. Note the careful verb: plausibly. The mechanism is real; the proof that eating this way changes vitiligo outcomes in humans is thin, and mostly comes from supplement trials layered on top of phototherapy (§6), not from food-diary studies.
3. Deficiencies worth correcting — the highest-yield move.
This is where diet-adjacent action has the firmest ground. Two deficiencies are reproducibly over-represented in vitiligo, and both are cheap to test and safe to correct.
Vitamin D.
Two independent meta-analyses confirm that people with vitiligo have lower serum 25-hydroxyvitamin D than controls. Upala & Sanguankeo pooled seven studies (1,200 patients) and found a mean difference of about −7.45 ng/mL[7]; the larger ViViD meta-analysis of 31 studies reached the same conclusion and noted the gap was widest in people who work indoors[8]. Important caveat: association is not causation. Low vitamin D may contribute to immune dysregulation, or it may simply reflect that people with visible depigmentation avoid the sun. Either way, checking 25-OH-D and replacing a genuine deficiency to a normal level is standard, low-risk, and reasonable — it is not a license to megadose.
Vitamin B12 and folate.
Vitiligo clusters with pernicious anemia (autoimmune B12 deficiency), so screening B12 and folate has a built-in rationale. The most-cited intervention is Juhlin & Olsson's two-year study of 100 patients on oral folic acid + B12: clear repigmentation in 52, with the best results in those who also got summer sun[9]. Read it honestly — it was uncontrolled, and the sun exposure is a confounder doing real work. When B12 + folate were added to controlled NB-UVB phototherapy, they produced no additional benefit over phototherapy alone[10]. The takeaway: test B12 and folate, correct a true deficiency, but don't expect supplementation on its own to repigment skin.
| Nutrient | Why it's on the list | Food sources | The honest verdict |
|---|---|---|---|
| Vitamin D | Lower in vitiligo across two meta-analyses[7,8] | Sunlight, oily fish, fortified dairy, egg yolk | Test; replace a real deficiency to normal. Don't megadose. |
| Vitamin B12 + folate | Pernicious-anemia overlap; classic (uncontrolled) repigmentation report[9] | B12: meat, fish, dairy, eggs (or supplement if vegan). Folate: leafy greens, legumes | Test; correct deficiency. No added benefit on top of phototherapy[10]. |
| Zinc & copper | Cofactors in melanin synthesis; cited often online | Zinc: shellfish, meat, legumes. Copper: nuts, seeds, shellfish | Evidence is conflicting — some studies show deficiency, others excess[4]. Don't supplement without a measured low. |
| Selenium | Antioxidant cofactor (glutathione peroxidase) | Brazil nuts, fish, eggs, whole grains | Plausible but unproven. Toxic in excess — never supplement blindly. |
4. The eating pattern that makes sense — antioxidant-rich, anti-inflammatory.
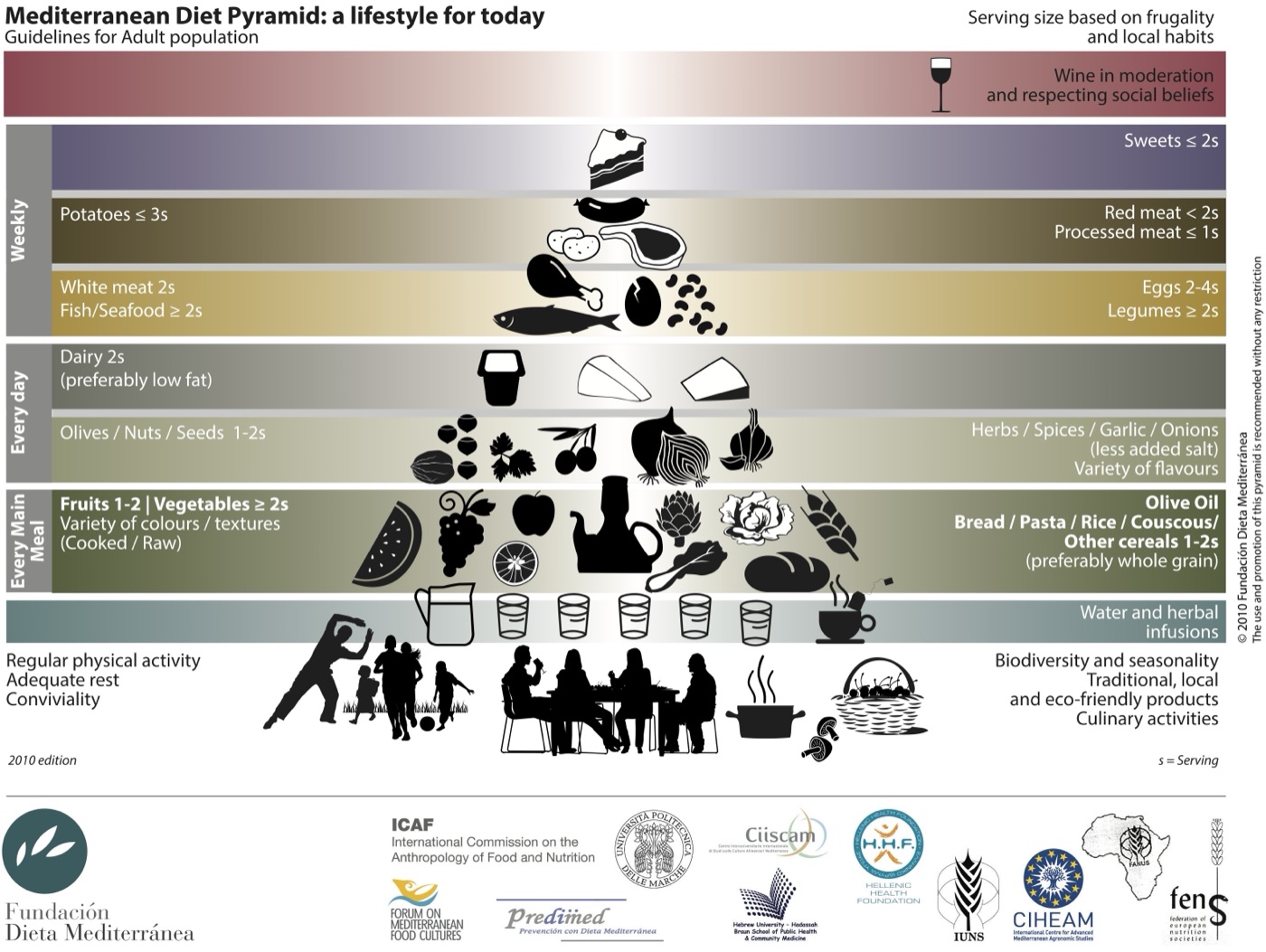
If diet's mechanism is "lower the oxidative load" (§2), then the dietary pattern follows directly — and it's the same boring, evidence-backed pattern that's good for nearly every chronic condition: a Mediterranean-style, antioxidant-rich, anti-inflammatory diet. Plenty of vegetables and fruit (especially colourful, polyphenol-dense ones — berries, leafy greens, peppers, onions), olive oil, oily fish, legumes, nuts and seeds; minimal ultra-processed food, deep-fried food, and excess alcohol[5,6].
The 2025 Nutrients review highlights antioxidant-rich foods — apples, green tea, Indian gooseberry (amla), onions, peppers — as plausibly helpful for lowering oxidative stress, while being explicit that this remains exploratory and shouldn't be sold as treatment[6]. That's the right framing. You're not eating to repigment a patch; you're eating to reduce the background oxidative tone the disease feeds on, and getting general cardiometabolic benefit as a bonus.
One honest limitation: there is no randomised trial of "the Mediterranean diet for vitiligo." The recommendation is an extrapolation from the oxidative-stress mechanism plus the supplement-trial data in §6 — not a tested protocol. It's a sensible default, not a proven cure.
5. The gut–immune angle — plausible, early, not proven.
Vitiligo sits inside a broader autoimmune cluster (thyroid disease, type 1 diabetes, alopecia areata), and the gut microbiome shapes immune regulation across that whole cluster. The logic — a more diverse, fibre-fed microbiome supports immune tolerance — is sound in general, and it's why fibre and fermented foods keep coming up in vitiligo diet discussions[4,6].
But be precise about the evidence grade: the gut–vitiligo link is mechanistic and associative, not trial-grade. There is no randomised trial showing that a fibre-rich or probiotic-rich diet changes vitiligo activity or repigmentation. So treat it as low-cost, low-risk background that's good for you anyway — diverse plants, legumes, whole grains, a little fermented food — and not as a treatment with an expected pigment payoff.
For the full mechanism on how the microbiome shapes autoimmune risk, the companion Gut Microbiome guide goes deep with the same standard of evidence used here.
6. Supplement adjuncts with actual trial data.
Here's the part most diet articles get backwards. A handful of supplements do have randomised evidence in vitiligo — but the consistent finding is that they work only as add-ons to phototherapy, not on their own. If you're not doing NB-UVB or a topical, these have little reason to help.

Polypodium leucotomos (oral fern extract).
An antioxidant, photoprotective fern extract. In a 2007 randomised double-blind placebo-controlled trial (50 patients), adding oral P. leucotomos to NB-UVB produced a trend toward more head-and-neck repigmentation (44% vs 27%), strongest in lighter skin types and in people who attended >80% of sessions — though it fell just short of statistical significance[11]. A 2021 RCT (44 patients) was cleaner: NB-UVB + PL gave a 47.8% response rate vs 22% for NB-UVB alone[12]. Promising as an adjunct; useless to expect as a standalone.
Antioxidant pools (vitamins C + E, alpha-lipoic acid).
Dell'Anna's 2007 double-blind RCT gave a balanced antioxidant pool (alpha-lipoic acid, vitamins C and E, polyunsaturated fatty acids) for 2 months before and 6 months during NB-UVB: 47% of the antioxidant group hit >75% repigmentation vs 18% on placebo[15]. A 2018/2021 systematic review and meta-analysis of antioxidant-plus-phototherapy RCTs found a modest but real benefit overall — again, as an add-on to phototherapy[16]. Single antioxidants in isolation (e.g. alpha-lipoic acid alone) generally did not work; the benefit, where present, came from combinations layered on UVB.
Ginkgo biloba.
The one supplement with a hint of standalone signal — for stabilising, not dramatically repigmenting. A double-blind placebo-controlled trial (47 patients, 40 mg three times daily) showed significant arrest of disease progression and marked-to-complete repigmentation in 10 of the treated group vs 2 on placebo[13]. A small 2011 open-label pilot (60 mg twice daily, 12 weeks) stopped progression in all 12 participants with an average ~15% repigmentation[14]. Small studies, mostly limited/slow-spreading disease — worth a conversation with your dermatologist, not a self-prescription.
7. What the evidence does not support.
The vitiligo internet is full of confident diets with nothing behind them. Naming them matters as much as naming what works.
- Gluten-free diet. There is no evidence that going gluten-free helps vitiligo in people who don't have celiac disease. The reviews are explicit that no vitiligo-specific diet has been formally validated, and gluten's role remains an open question, not an established one[3,6]. If you have coexisting celiac disease, treat the celiac — otherwise, eliminating gluten is unsupported.
- "Copper-rich miracle" foods and copper supplements. Copper is a melanin cofactor, which fuels the myth — but the trace-mineral evidence is conflicting (deficiency in some studies, excess in others)[4], and copper is toxic above a fairly low ceiling. No controlled evidence supports copper loading.
- Anti-Candida, "alkaline", and detox diets. No mechanism, no trials, no support in any review[3,4,5,6]. These are general-wellness folklore mapped onto vitiligo.
- Blanket elimination diets. Cutting whole food groups "just in case" carries real downside — nutrient gaps, disordered eating, social cost — with no demonstrated vitiligo benefit. (The Autoimmune Protocol is a structured, time-limited version with its own thin evidence base; see the AIP guide for an honest read — it has never been studied in vitiligo specifically.)
8. A few real nuances — heavy metals, phenylalanine, and the vitamin C caveat.
Heavy-metal exposure. The 2024 systematic review flagged a signal that exposure to cadmium, lead, and mercury correlates with higher reactive-oxygen-species load and vitiligo risk[4]. This is an environmental/oxidative-stress point, not a "diet" lever you optimise — but it reinforces the same theme: keep the oxidative burden down.
Phenylalanine. An amino acid that's a precursor in melanin synthesis. Some older work paired oral L-phenylalanine with UVA and reported benefit[5]; it's a supervised, phototherapy-paired protocol if used at all — not a food you add to dinner for pigment.
The vitamin C caveat. Vitamin C is a useful dietary antioxidant and part of the antioxidant pools that helped alongside UVB (§6) — but very high-dose vitamin C can interfere with melanin formation (it's used cosmetically to lighten skin). The practical read: dietary and normal supplemental vitamin C is fine and probably helpful as part of the antioxidant picture; megadose vitamin C is not a vitiligo strategy and is theoretically counterproductive.
9. Your diet & nutrient self-audit.
Fifteen items mapped to the levers above. Tick what's true for you. Instead of a single score, the panel shows a profile across four lanes — deficiency risk, oxidative/dietary load, gut-immune support, and readiness — and surfaces the honest next steps (which labs to ask for, where diet realistically helps, and where it won't). Nothing is sent anywhere; it's saved only to your own browser so you can revisit and update it.
Tick what's true for you. Instead of a single score, the panel below shows a profile across four lanes — deficiency risk, oxidative/dietary load, gut-immune support, and how ready you are to act — and surfaces the honest next steps (mostly "test, don't guess" and "adjuncts only help alongside phototherapy"). Saved to this browser only; nothing is submitted anywhere.
Your pattern already covers the basics. Remember the honest bottom line: no diet cures vitiligo. Keep the antioxidant-rich pattern, correct any measured deficiency, and put your energy into the treatments with real evidence.
References.
Every PMID below has been verified against PubMed before this page was committed. Click any number in square brackets above to jump to its entry below; click "PubMed" to open the paper.
- Picardo M, Dell'Anna ML, Ezzedine K, Hamzavi I, Harris JE, Parsad D, Taieb A. Vitiligo. Nat Rev Dis Primers. 2015;1:15011. PubMed: 27189851
- Schallreuter KU, Salem MA, Holtz S, Panske A. Basic evidence for epidermal H2O2/ONOO(-)-mediated oxidation/nitration in segmental vitiligo is supported by repigmentation of skin and eyelashes after reduction of epidermal H2O2 with pseudocatalase. FASEB J. 2013;27(8):3113–3122. PubMed: 23629861
- Grimes PE, Nashawati R. The Role of Diet and Supplements in Vitiligo Management. Dermatol Clin. 2017;35(2):235–243. PubMed: 28317532
- Hadi Z, Kaur R, Parekh Z, Khanna S, Bin Khalil AB, Abbasi HQ, Ashfaque F, Shah D, Patel VJ, Al Hasibuzzaman M. Exploring the impact of diet and nutrition on vitiligo: A systematic review of dietary factors and nutritional interventions. J Cosmet Dermatol. 2024;23(7):2320–2327. PubMed: 38465786
- Dutta RR, Kumar T, Ingole N. Diet and Vitiligo: The Story So Far. Cureus. 2022;14(8):e28516. PubMed: 36185835
- Diaz MJ, Tran JT, Rose D, Wei A, Lakshmipathy D, Lipner SR. Dietary Interventions, Supplements, and Plant-Derived Compounds for Adjunct Vitiligo Management: A Review of the Literature. Nutrients. 2025;17(2):357. PubMed: 39861486
- Upala S, Sanguankeo A. Low 25-hydroxyvitamin D levels are associated with vitiligo: a systematic review and meta-analysis. Photodermatol Photoimmunol Photomed. 2016;32(4):181–190. PubMed: 27005676
- Varikasuvu SR, Aloori S, Varshney S, Bhongir AV. Decreased circulatory levels of Vitamin D in Vitiligo (ViViD Study): a meta-analysis. An Bras Dermatol. 2021;96(3):284–294. PubMed: 33863565
- Juhlin L, Olsson MJ. Improvement of vitiligo after oral treatment with vitamin B12 and folic acid and the importance of sun exposure. Acta Derm Venereol. 1997;77(6):460–462. PubMed: 9394983
- Tjioe M, Gerritsen MJ, Juhlin L, van de Kerkhof PC. Treatment of vitiligo vulgaris with narrow band UVB (311 nm) for one year and the effect of addition of folic acid and vitamin B12. Acta Derm Venereol. 2002;82(5):369–372. PubMed: 12430737
- Middelkamp-Hup MA, Bos JD, Rius-Diaz F, Gonzalez S, Westerhof W. Treatment of vitiligo vulgaris with narrow-band UVB and oral Polypodium leucotomos extract: a randomized double-blind placebo-controlled study. J Eur Acad Dermatol Venereol. 2007;21(7):942–950. PubMed: 17659004
- Pacifico A, Damiani G, Iacovelli P, Conic RRZ, Gonzalez S, Morrone A. NB-UVB plus oral Polypodium leucotomos extract display higher efficacy than NB-UVB alone in patients with vitiligo. Dermatol Ther. 2021;34(2):e14776. PubMed: 33433041
- Parsad D, Pandhi R, Juneja A. Effectiveness of oral Ginkgo biloba in treating limited, slowly spreading vitiligo. Clin Exp Dermatol. 2003;28(3):285–287. PubMed: 12780716
- Szczurko O, Shear N, Taddio A, Boon H. Ginkgo biloba for the treatment of vitiligo vulgaris: an open label pilot clinical trial. BMC Complement Altern Med. 2011;11:21. PubMed: 21406109
- Dell'Anna ML, Mastrofrancesco A, Sala R, Venturini M, Ottaviani M, Vidolin AP, Leone G, Calzavara PG, Westerhof W, Picardo M. Antioxidants and narrow band-UVB in the treatment of vitiligo: a double-blind placebo controlled trial. Clin Exp Dermatol. 2007;32(6):631–636. PubMed: 17953631
- Jung HM, Jung YS, Lee JH, Kim GM, Bae JM. Antioxidant supplements in combination with phototherapy for vitiligo: A systematic review and meta-analysis of randomized controlled trials. J Am Acad Dermatol. 2021;85(2):506–508. PubMed: 30342161
Related on Aayushnitya
- The Vitiligo Guide →
The disease itself — the IFN-γ/CXCL10 immune attack, subtypes, and the treatments that actually move VASI scores (ruxolitinib cream, oral JAK inhibitors, NB-UVB, surgical grafting). Read this for what works; this diet guide is the supporting cast.
- Gut Microbiome Guide →
The gut–immune mechanism behind the §5 angle, with the same evidence standard — how the microbiome shapes autoimmune risk, and what to eat (and why).
- The AIP Diet Guide →
An honest read on the Autoimmune Protocol elimination diet — its leaky-gut rationale, the small IBD/Hashimoto's pilots, the real risks, and why it has never been studied in vitiligo (§7).
- Ferritin Interpreter →
Ferritin, B12, and the anemia that travels with vitiligo cluster together (§3). Part of the same baseline lab panel worth running before you supplement anything.
This guide is a synthesis of peer-reviewed research and is not medical advice. Diet does not cure vitiligo. Diagnosis and treatment — including phototherapy, topical drugs, and any supplement used alongside them — require evaluation and supervision by a qualified dermatologist. Test before supplementing; correct measured deficiencies to a normal level, not beyond. The interactive audit is a discussion aid for your clinician visit, not a diagnostic instrument.